


Covid and the Golly Folly
The blind spot of gee whiz technology futurism: Part 12

“Optimism is, in the first instance, a way of explaining failure, not prophesying success.” – David Deutsch, The Beginning of Infinity
When it comes to Covid, most of the supposedly high-information policy world is still living two to three years behind the cutting-edge science and data. Covid censorship and propaganda (or CCP, no pun intended) was extraordinarily effective. We recently argued as much in The Wall Street Journal. CCP was surprisingly potent in the very communities which should have had the analytical tools to resist its charms and misdirections.
For some reason, regular people slowly figured things out. Yo, Canadian truckers! Examples keep rolling in, however, showing those most vulnerable to the infowarp were experts in public health and the wider public policy world.
The latest is an item from Richard Hanania, a social scientist who writes mostly about culture and discrimination law, including a new book called The Origins of Woke. I wouldn’t have noticed or replied here except that I saw smart people citing his new article as a successful vindication of the Covid vaccines. Another sigh-inducing item is from Harvard psychologist Steven Pinker, author of Enlightenment Now and Rationality, among other good books. Pinker still thinks SARS2 first jumped to humans in a wet market. A third example comes from economist Tyler Cowen, who believes China’s zero-Covid lockdowns worked and maybe the country should still be closed until it adopts mRNA technology. All three demonstrate the folly of cursory cheerleading, rather than deep scientific analysis.
Most would understandably prefer to move on from Covid. But the issues are simply too important. Increasingly powerful biotechnologies, and thus bioethics, will dominate policy discussions in coming years. We need to understand what happened during Covid, and we need accountability. Even more generally, our sense-making institutions, which promote individual and collective information processing and good decisions, are broken. They must be returned to health or replaced with better ones.
These three examples also highlight another growing problem – the superficiality of analysis by some in the pro-innovation “progress studies” universe. Their hearts are almost always in the right place. Their brains, too, for the most part. I share their enthusiasm for exuberant, technology-led economic growth. Progress in biotech, energy, and other fields should be a central objective of our civilization.
The moniker of “technology,” however, is never decisive. Labeling windmills “green energy” does not make them a greener or more efficient electricity source than natural gas or nuclear power. Modern medicine’s ability to interrupt puberty does not mean lots of 12-year olds should indulge in, nor doctors push, extreme hormone therapy. Likewise, the label “vaccine” does not tell you anything about a medicine’s underlying biology or its safety and effectiveness.
In fact, skipping over the details may, by leading to or excusing (or covering up) catastrophic mistakes, undermine the bigger mission of technological progress. As we’ve seen with nuclear power, even one innocuous misstep (Three Mile Island) and one real disaster (Chernobyl) can set back a crucial technology for decades.
Let’s address the examples and then return to bigger themes.
Risk and Benefit Reversed
Hanania’s biggest point is that “the public health establishment is too risk averse.”1
At one level, that’s absolutely true. Public health showed extreme risk aversion when it came to the virus itself. After all, they convinced the world to close down for several years. Lockdowns devastated economies and social health without stopping the virus.
Hanania acknowledges we may have overdone it with lockdowns and school closures. And yet later on, he asserts that Covid was even more dangerous than the panic-stricken media and public health officials argued – “we’ve been undercounting, not overcounting, how bad the disease has been.” And not just for the elderly. “[E]ven for the young,” he argues, “covid was a big enough problem that it was worth it to get two shots.”
Hanania’s real criticism regarding risk aversion, therefore, is not about lockdowns or over-hyping Covid; he basically agrees with public health’s extreme worry over Covid severity. It’s that we should have even more aggressively deployed mRNA vaccines. If only public health had more fully embraced a miracle technology, he says, we might have saved more people from a devastating disease.
Hanania’s risk-aversion arguments, however, are backwards.
First, the Covid-19 vaccine roll-out was by far the largest, fastest, broadest medical intervention in world history. All previous vaccines took many years to develop and test, and decades to deploy. It’s difficult to fathom how they could have been more aggressive – many billions injected within two years of viral emergence – save for the politically motivated delay of two weeks to push the shots beyond the 2020 election.
A bigger point is that the mRNA vaccines are a radically new technology. They genetically transfect our cells with three novel components – lipid nanoparticles, which deliver modified synthetic mRNA, which codes for an engineered foreign Spike protein. The mRNA platform may be ingenious. Future mRNA iterations may be successful. The Covid mRNA vaccines, however, were anything but low-risk. Public health embraced risk as never before.
Public health inverted the risk-benefit equation, leading to widespread miscalculation of potential benefit and harm. For the broad population, health officials and Pharma told us Covid was high-risk and genetic transfection was low-risk. It appears now just the reverse was true.
But how do you know our risk-benefit analysis is better than the conventional narrative Hanania embraces? Our point is that the progress crowd didn’t do its homework. We thus need to demonstrate, rather than merely assert, these points.
Real Science, Real Data
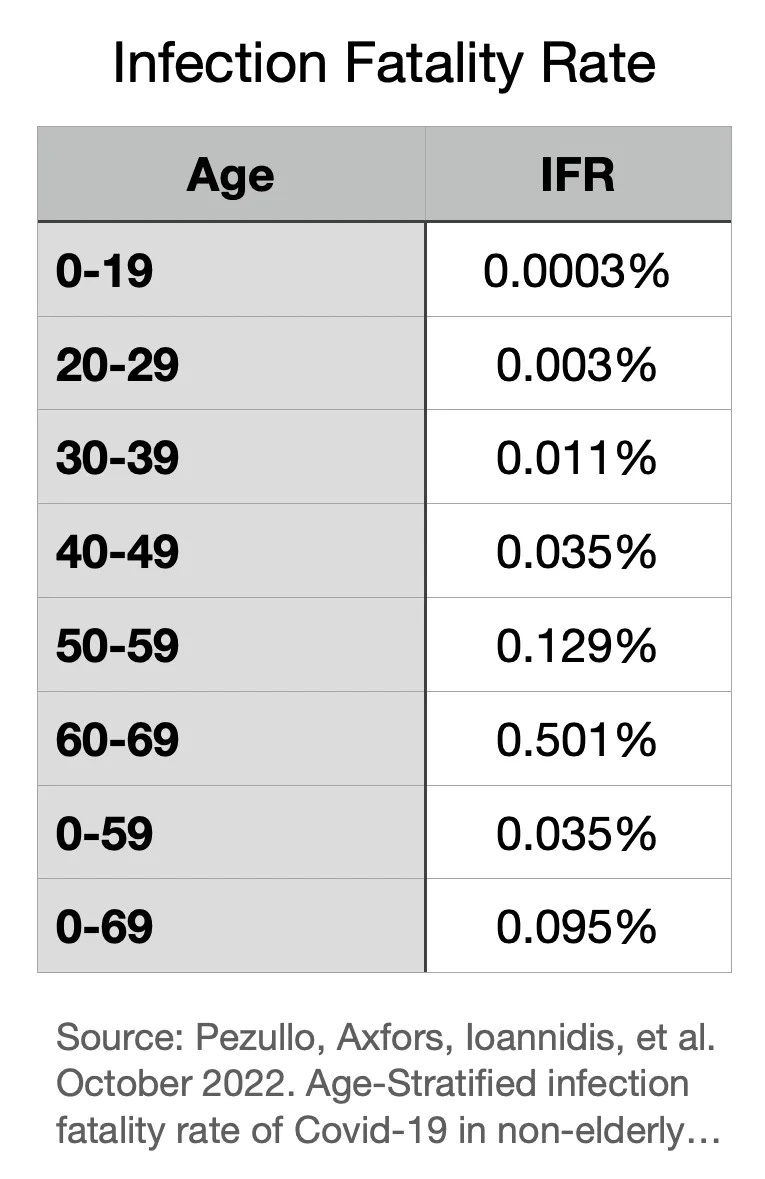
A central fact of Covid was extreme risk stratification by age. Despite Hanania’s assertion that Covid was more dangerous than assumed, even for young people, vast amounts of global data show most people under 70 were at little risk (see, Ioannidis, et al., below). Large numbers of deaths misattributed to Covid were the result of lockdowns and iatrogenic harms.
Given the vast majority of people were at low risk for Covid, why would public health embrace and mandate a potentially high-risk treatment?
One plausible argument for widespread vaccination was that it would protect the vulnerable. Blocking infection would generate herd immunity. The only remotely plausible argument for vaccine mandates was that, even failing a private benefit, they would offer a public benefit.
Hanania still argues this point: Covid vaccines “make transmission somewhat less likely by preventing infections in the first place.” And, “It is true that efficacy wanes over time. The answer to this seems to be boosters, which also work.”
Beginning in autumn 2021, we knew just the opposite is true. Unfortunately, more doses equal more infections.
The Cleveland Clinic, for example, studied its 51,011 employees and showed negative effectiveness. Every shot, in fact, boosts one’s risk of Covid infection. Four shots is worse than 3, is worse than 2, is worse than 1, is worse than none.
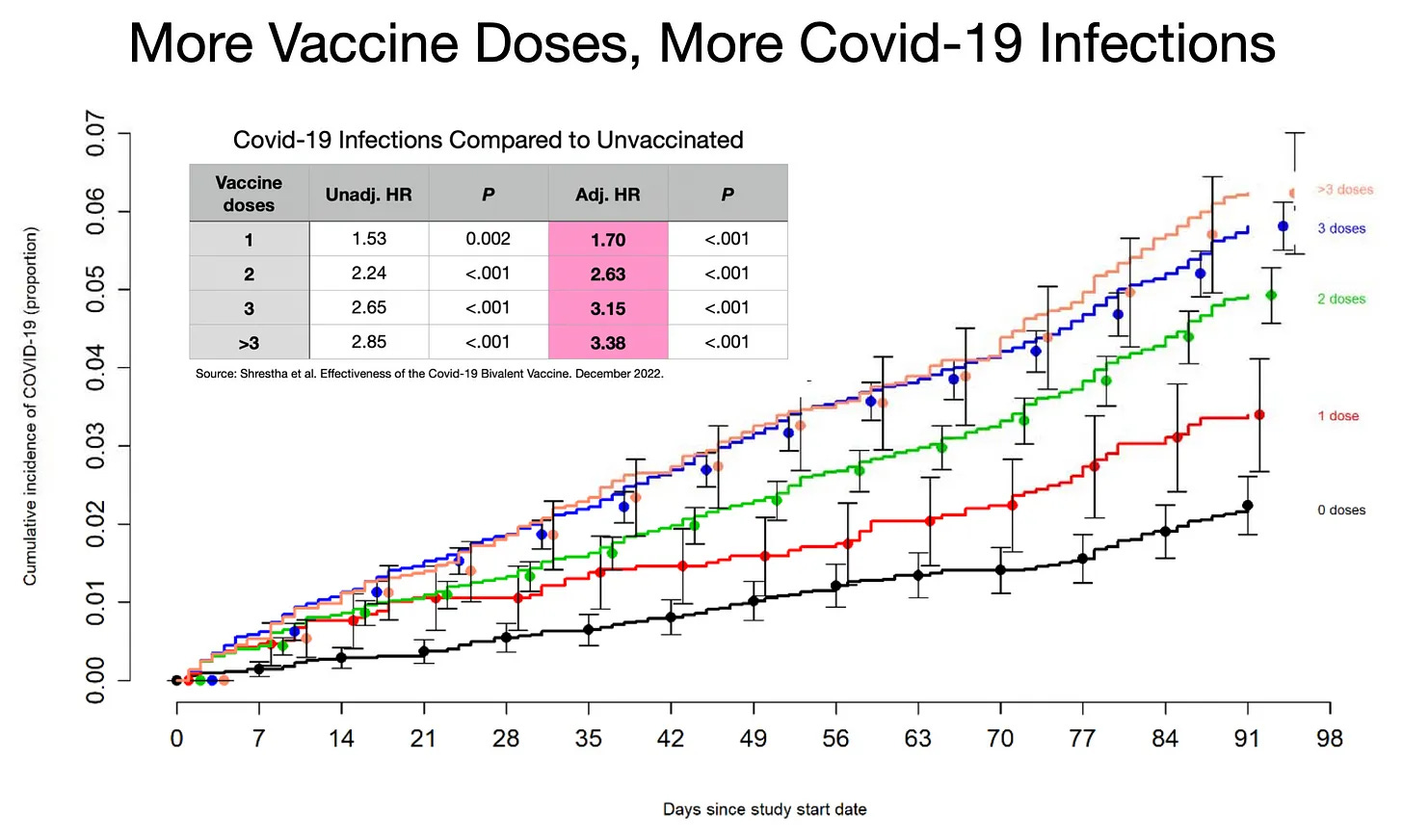
In a follow-up study, the Cleveland Clinic found that its employees who were “up to date” on their vaccinations were worse off than those “not up to date.” Our article More Vaccine Doses, More Infections speculates about the likely biological causes of this counterintuitive effect – immune imprinting and tolerance.
Mass deployment of leaky vaccines, paradoxically, extended the pandemic by several years. By exerting extreme evolutionary pressure, the strategy selected for more infectious, vaccine-evading variants. Instead of herd immunity against the virus, we generated herd opportunity for the virus. So much for any public benefit.
What about private protection against disease and death? Don’t the Covid vaccines at least protect individuals from getting sick and dying? Hanania repeats the conventional wisdom they do. Like so much since 2020, however, big assertions based on narrowly tailored and often inscrutable analysis (or, more often, mere talking points) cannot overcome the elephant in the vial.
At the highest level, the assertion the Covid vaccines prevented severe disease and death cannot be squared with the explosion of morbidity and mortality around the high-income world in 2021, 2022, and 2023. See Germany as a representative example.
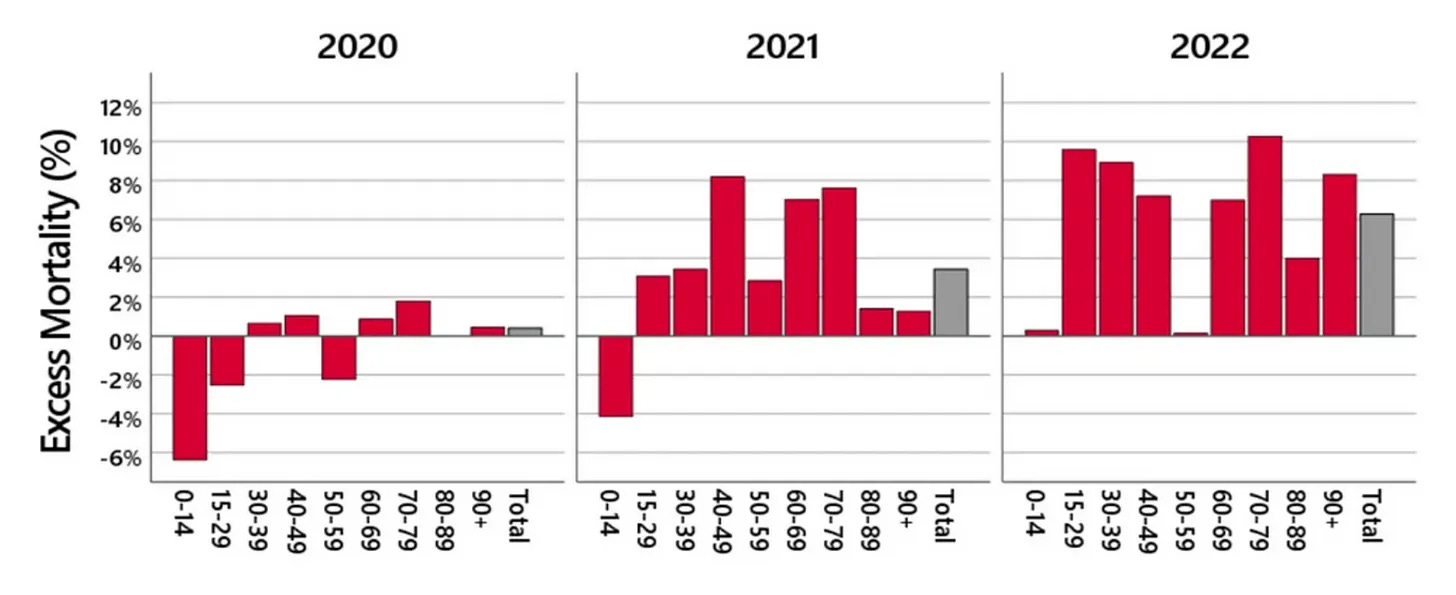
This surge occurred most conspicuously among young and middle-age healthy people, though the elderly continue to suffer at high rates, too. We recently surveyed the U.S. and global experiences, including life insurance data, in numerous articles:
Where Did All the Workers Go?: A U.S. Mortality Survey: Part 5
Society of Actuaries Shows Continued Young Adult Mortality Spike: Part 10
Hanania and many others often hang their vaccine effectiveness hats on a particular chart compiled using CDC data. The chart appears to show a dramatic spike of deaths among the unvaccinated in late 2021 and early 2022. But we showed months ago that because of several major miscounting and modeling errors, the data used in the chart is invalid.
Newer data released by the UK’s Office of National Statistics reconfirms our analysis. Sadly, it also shows all-cause mortality among vaccinees, adjusted for age and time, is generally higher than for the unvaccinated.

UK data is far from perfect but exceeds the quality and uniformity of U.S. data.2 The chart above probably underestimates the number of unvaccinated Brits and does not correct for healthy vaccinee bias. The chart therefore represents the best case for vaccine effectiveness. The truth might be even worse. Most people of all ages, therefore, would probably have been better off avoiding vaccination.
Disability Surge
Hanania vaguely blames Covid and Long Covid for astonishing rises in disability. But he offers no mechanism by which (Long) Covid begins causing neurological, cardiac, clotting, cancer, and autoimmune problems among often young and healthy people in 2021, reaching unprecedented levels in 2022-23, but not in 2020.
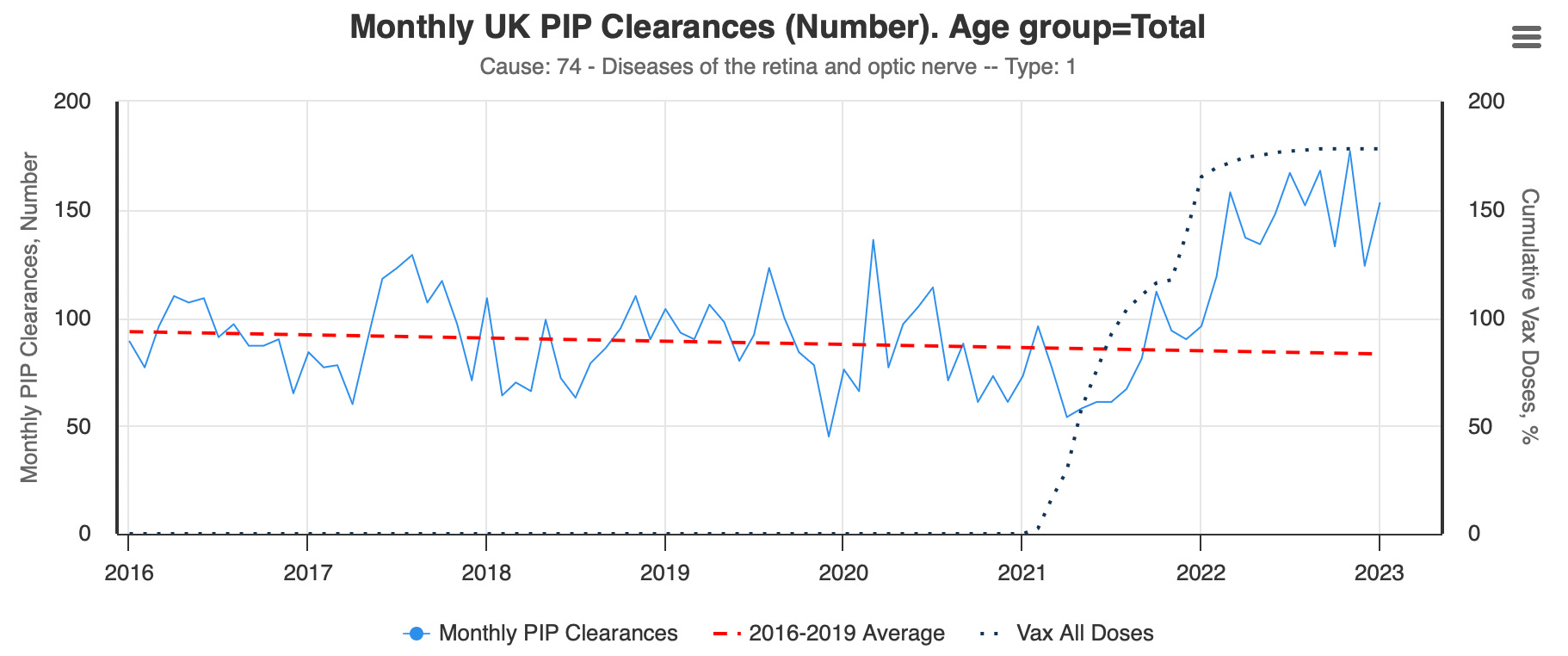
By contrast, Ed Dowd’s new analysis of UK disability data from the Personal Independence Pension system explodes with highly specific temporal and organ system signals in 2021-23. (Dowd is a former BlackRock portfolio manager.) The labels in the charts below are hard to see, so, in descending order, they show monthly disability claims approved by the UK government for blood disorders, cardiac failure, retina and optic nerve diseases, neuropathy (e.g., nerve pain and tingling), and cerebrovascular (e.g., stroke). I’ve selected just five among dozens of specific disorders; you can see the comprehensive data on Dowd’s website.




The Basic Biomechanism
Why is it so difficult for most smart people, who appreciate biomedical innovation in general and traditional vaccines in particular, to contemplate the possibility the novel mRNA vaccines might not be safe and effective? Their admirable pro-technology orientation may be one factor. Or perhaps they cannot fathom these problems because they’ve not studied the physiology of the mRNA shots.
Here’s a summary:
A single vaccine dose contains more than one trillion lipid nanoparticles (LNPs), or tiny fat bubbles, which envelope tens of trillions of modified mRNA strands. The LNPs deliver mRNA into cells in organs all over the body. Pharma companies and health authorities hoped and told us the vaccines (a) stayed in our shoulder muscles and (b) degraded in hours or days. Not so; they often spread throughout our bodies and remain for many weeks or months.
Cells read the mRNA, translate the code, produce the Spike protein, and express Spike on their surfaces. Mimicking a natural infection, this artificial infection is called transfection. Among other important distinctions, the vaccine bypasses the body’s first lines of defense – our powerful mucosal immune system in our upper-respiratory and digestive tracts. Where most natural SARS2 infections will be defeated in our noses and throats, often in several days, before the virus spreads into the deep lung or rest of our bodies, the vaccines deliver vast quantities of the Spike code deep behind enemy lines.
The Spike protein itself is harmful. It irritates and damages endothelial cells (the inner lining of blood vessels) and causes inflammation and clotting among other pathologies. But there’s an even more basic problem.
Our immune systems target transfected cells for destruction. The fundamental concept governing immunity is self/non-self, or native and foreign. Our immune systems ignore native substances and kill foreign ones. Like the SARS2 Spike, the vaccine Spike is a foreign protein. Our immune systems recognize the foreign Spike protein and react. Over several weeks, we develop antibodies against Spike, preparing for the next SARS2 encounter. (This adaptive memory response is what we hear about in the news; it’s how the vaccines are intended to work.) Even before that, however, we deploy a more immediate response. A foreign antigen signifies infection (transfection) and calls upon our white blood cells, such as killer T cells and natural killer (NK) cells, to destroy the compromised cells.
Destroyed muscle cells in your shoulder may cause pain. No big deal. But when the mRNA vaccines transfect heart cells, nerve cells, or endothelial (vascular) cells in important tissues, the damage can be severe or even catastrophic. If, for example, too many cells lining the aorta are transfected, it can cause arteritis and possibly aortic dissection and instant death. These events are not speculative. We have the autopsies to prove the bio-mechanisms.
Most drugs are metabolized, degraded, and/or secreted. But mRNA is not merely a chemical; it’s a code. As long as the code remains, our ribosomes will read it and make Spike. Because the LNPs often spread throughout the body, and because the mRNA modified with pseudouridine (Ψ) might not break down but remain active, cells in many important organs can transfect and generate potentially large quantities of Spike for long periods of time (at least six months, according to this study). It’s often said, “The dose makes the poison.” But unlike most drugs, we don’t know how much Spike protein a given amount of modified mRNA generates. We therefore don’t know the actual dose. This might be one reason adverse events associated with these vaccines are so numerous, long-lasting, and diverse, from skin rashes to nerve tingling, from myocarditis to stroke to endless immune dysregulation. It also means that mRNA products coding for any foreign protein, not just Spike, might exhibit many of the same problems.
Our long Twitter thread on myocarditis cites dozens of published studies detailing the pathophysiology and seriousness of vaccine-induced heart inflammation. It also distinguishes between myocarditis caused by SARS2 infection (extremely rare) and vaccination (far too common). German pathologist Arne Burkhardt’s autopsies are instructive. He and 10 international colleagues performed 75 second-opinion autopsies of post-vaccine deaths. Thirty-one of the 75 were originally labeled sudden cardiac deaths with uncertain cause. Upon deeper examination, however, Burkhardt et al. found, of those 31 cardiac deaths, 15 were due to vaccine-induced myo/pericarditis, while 16 were caused by vaccine-induced “microangiopathy” with stenosis and/or dissection of the heart vessels, including the aorta. They found both vaccine Spike and lymphocytes in the damaged tissues. This and similar case series may help us understand the major rise in cardiac problems and sudden deaths (SADS) over the last two-plus years. Because myocarditis often scars the heart, it can substantially elevate risk of arrhythmias and other severe heart complications for years or decades to come.
We don’t yet understand all the pathways, but it appears the mRNA vaccines may also promote cancer. Possible mechanisms include suppression of our immune surveillance networks which constantly find and kill (pre-)cancerous cells; interruption of our DNA-repair mechanisms, such as the TP53 gene, known as the “guardian of the genome”; and potentially even DNA contamination within the LNPs, as described by genomicist Kevin McKernan and confirmed independently by “cancer gene jock” Phillip Buckhaults, a professor at the University of South Carolina.3
If one grasps this pathophysiology, the extraordinary mortality and morbidity in the high-income world makes sense. So does the explosion of adverse events detailed in the Vaccine Adverse Event Reporting System, or VAERS. If one doesn’t understand the bio-mechanisms, all these numbers will seem implausible, and “Long Covid” will be the unsatisfying fallback.
Hanania, accordingly, repeats the lazy line that because anyone can report a vaccine injury, VAERS is invalid. In fact, health professionals submit more than 80% of reports. Regardless, the CDC then follows up to validate reports before elevating them to the public database.
As an early warning system, VAERS is far from perfect; so imperfect that it undercounts most events by at least a factor of 10 and sometimes a factor of 100. In the case of Covid, even the undercounted numbers were so outrageously large, it did its job – detecting more than 700 varied types of blaring safety signals. These warning flares normally would have elicited further investigation with emergency speed. And yet officials not only ignored the hundreds of obvious five-alarm blazes. They disavowed the nation’s chief safety surveillance tool.
Independent sources agree with VAERS. V-Safe, for example, a brand new app-based program set up specifically for the Covid vaccine rollout, confirms the VAERS safety signals. Once pried open by FOIA lawsuits, we found that of the 10 million people who voluntarily signed up for V-Safe, 770,000, or 7.7%, suffered adverse reactions severe enough to send them to a doctor or hospital for treatment. Europe’s EudraVigilance system, UK’s Yellow Card system, and the Pentagon’s DMED database also corroborate VAERS and each other.
Medical journals have now published more than 3,200 peer-reviewed case reports/series of deaths and severe injuries. The linked database shows that the vaccines cause devastating cardiac, neurological, vascular, and autoimmune problems. For each published report, where physicians took the time to write up and submit a case to a peer-reviewed journal, there are many thousands of similar unpublished incidents. Injuries from the mRNA vaccines may now total tens of millions worldwide.
Rah, Rah, Sis Boom Bah
Not to worry, Hanania, writes. Even if critics of the Covid policy response make a few good points, they are too hung up on details. They don’t see the bigger picture. We should praise big risk-taking efforts like the vaccine because they are “99% Good.”
In other words, technology generally points us in the right direction. So we should mostly go with it and not criticize. I agree technology is the key factor boosting living standards and human flourishing over time. I’ve spent the last 25 years arguing just that. Anti-tech pessimism is indeed a real problem retarding economic growth.
The general point, however, does not excuse lazy thinking and avoidable, catastrophic mistakes. “Progress” and “technology” are not get-out-of-jail free cards for historic blunders or tyrannical impositions.
True optimism requires intense criticism. Or as the great philosopher of science David Deutsch wrote, “Optimism is, in the first instance, a way of explaining failure, not prophesying success.” Optimists know tomorrow can be better than today – but only if we do the hard work of introspection and improvement.
Here, playing the “progress” card just means Hanania (1) didn’t do his homework on the biology and data of Covid and the vaccines; and/or (2) believes intentions are more important than results.
Such a flippant approach would overturn all of medical ethics. We don’t experiment on people, without their informed consent, for the greater good. Or because progress demands it. Or because technology is “99% Good,” as Hanania writes.
We don’t do it precisely because (1) it can cause irreparable harm to individuals, in this case millions, many of whom were at little risk. But also because (2) in this case, a worldwide experiment generated negative externalities by selecting for variants which extended the pandemic and harmed everyone. (More to come on this point, responding to NN Taleb’s multiple misapplications of the precautionary principle during Covid.)
Too many tech-progressives let their enthusiasm for innovation and hatred of red tape – perspectives I share – lead to premature conclusions. All speedy FDA approvals are good, they reflexively believe. I’ve recently made the distinction between a Right to Try and a Duty to Comply.
We could have achieved all the “innovation” and learning about the novel mRNA platform through responsibly executed clinical trials that were not prematurely unblinded. We didn’t need to inject several billion people while avoiding rigorous data collection and reporting.
Failing to critique the mRNA vaccines now may set back the platform’s future promise. If people do not believe we are learning from mistakes, they will not trust the technology.
We should be smart enough to hold two ideas at once. We can both (1) celebrate and practice technological innovation and (2) use our brains to conduct reasonable risk-benefit analyses, protect individual rights, and test highly novel experimental interventions before we urge or force billions to participate.
Take it a step further. In the name of “predicting and preventing” pandemics, EcoHealth Alliance and the Wuhan Institute of Virology, with hundreds of millions of dollars of support from U.S. government agencies, likely created the virus in the first place. But our next subject, Professor Pinker, does not want to believe technology may have caused the pandemic.
Enlightenment, Please
Like Matt Ridley’s book The Rational Optimist, Steven Pinker’s book Enlightenment Now makes a persuasive case for technology-based progress and why it makes sense to be optimistic. It’s a worthy entry in the catechism of innovation studies.
When he praised a new article in Quilette, however, Pinker joined many others in the clergy and demonstrated the years-long-lag in biological understanding.

The article claimed overwhelming evidence for a zoonotic, or natural, origin by reciting the familiar but unpersuasive stories about pangolins, raccoon dogs, and wet market stalls.
But it suffered the same devastating deficiencies of all the Zoo Crew analyses. Among them, it either casually waves away or totally ignores the most crucial facts suggesting SARS2 was engineered: (1) pre-pandemic research proposals to construct a virus exactly like SARS2; and (2) molecular analyses of the virus which point overwhelmingly to human tampering.
It’s difficult to take seriously any analysis which favors stories based on suspect Chinese wet market data but avoids the direct molecular evidence.
In 2021, the research group Drastic uncovered a 2018 grant proposal by EcoHealth Alliance to DARPA. EcoHealth sought to create a chimeric SARS-like virus, including an implanted furin cleavage site (FCS), which would dramatically boost infectivity in humans. The Quilette article claims because DARPA rejected the grant, no such work ever took place. Before that grant proposal, however, EcoHealth had for many years already been working on similar projects with North Carolina-Chapel Hill’s Ralph Baric and the Wuhan Institute of Virology. They published as much in 2015. One agency’s failure to fund a detailed blueprint is not evidence the blueprint was never employed. Finding a real-world replica of the blueprint, on the other hand…
In 2020, Dr. Steven Quay and others showed how the FCS contained an unnatural but human-optimized amino acid pair – CGG-CGG – which suggested laboratory engineering.
Then in an October 2022 pre-print, biologists Valentin Bruttel, Alex Washburne, and Antonius VanDongen described a molecular fingerprint suggesting a synthetic origin. As we previously wrote:
They showed that SARS2 appears to be stitched together just like other known experimental synthetic viruses.
Scientists use a technique known as in vitro genome assembly (IVGA) to create infectious clones. The technology cuts the virus genome into regular pieces, which can then be removed, replaced, and altered to explore new characteristics. These cutting sites – called restriction sites because of the restriction enzymes used to cut – offer a convenient map for plug-and-play genomics. Natural viruses also have restriction sites; but they do not have such regularly sized or spaced chunks of code.
Washburne and colleagues showed that previous plug-and-play experimentation with SARS-like clones all cut the virus into between five and eight fragments. The fragment lengths were similar, too, with no extremely long fragments. They predicted that SARS2 would fit into the red box of known synthetic viruses below, and bingo; it did. The trio also found SARS2 has a significantly higher portion of synonymous mutations in these restriction sites than its natural cousins.

In just the last month, biologist Jesse Bloom published an additional molecular argument. It points away from the supposed mid-December 2019 wet market animal origin and toward an earlier pre-December 2019 event. He concluded:
The first human infections with SARS-CoV-2 in Wuhan probably occurred no later than November 2019 (Zhang et al. 2020; van Dorp et al. 2020; He and Dunn 2020; Pipes et al. 2021; Pekar et al. 2021; ODNI 2022; Pekar et al. 2022), which is over a month before the Chinese CDC reports that it began to collect samples from the market.
So we now have a molecular fingerprint and a molecular timestamp suggesting SARS2 was engineered.
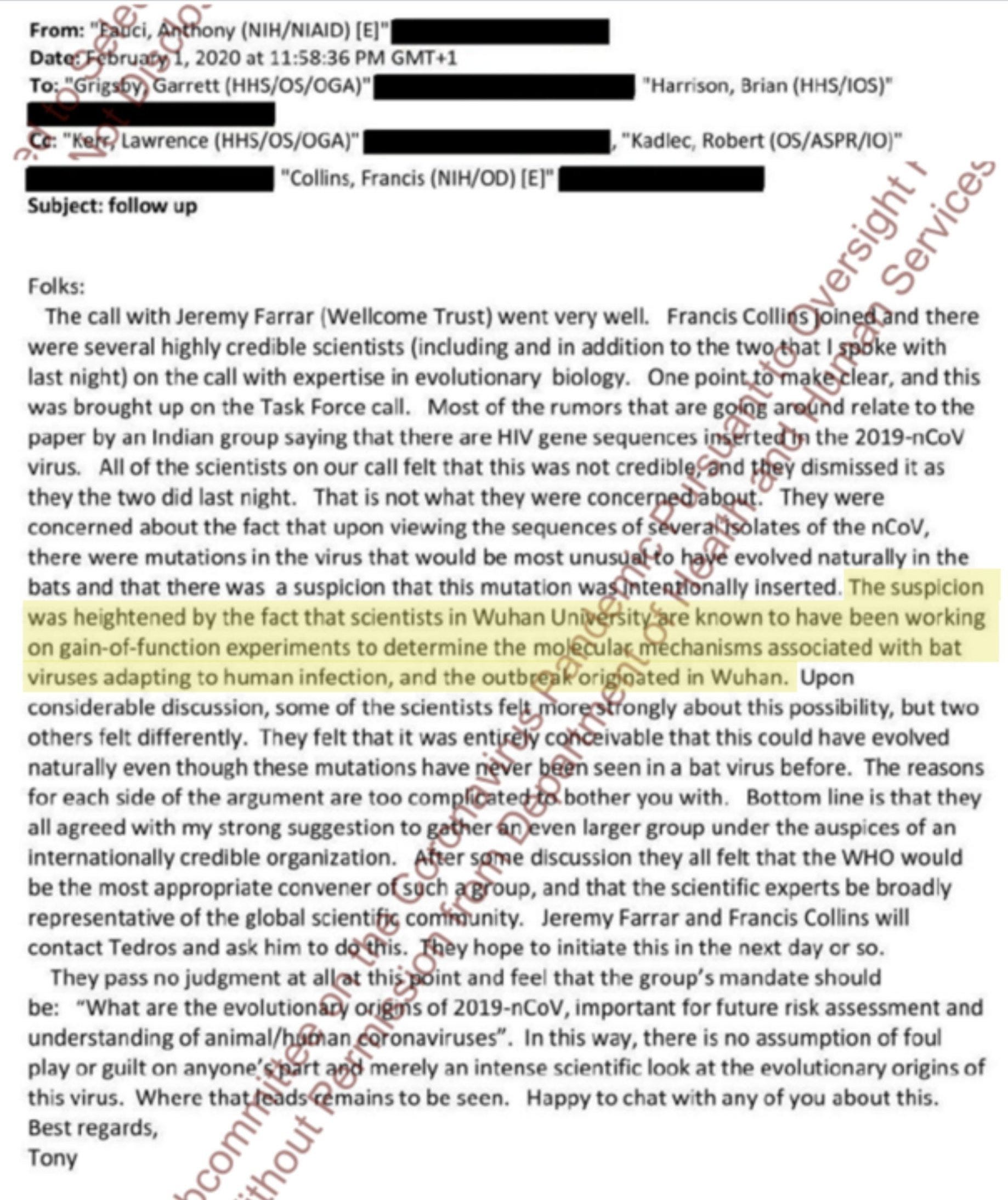
We also of course have Dr. Anthony Fauci’s own words, and those of his virologist posse, detailing their initial views the virus was engineered.4
The White Coat Test
I had not previously realized Pinker was so in thrall to Covid orthodoxy. Looking back, however, his passive allegiance is clear.
In January 2023, Pinker wrote that white lab coats were all he needed to obey.
For my part, I’ve been vaccinated against Covid five times, but my understanding of how the vaccines work extends little deeper than “Something something mRNA antibodies immune system.” I basically trust the people in the white coats who say they work. Flaky beliefs, in contrast, persist in people who don’t trust the public health establishment — who see it as just another faction, one that competes against their trusted preachers, politicians, and celebrities. In other words, we all have to trust authorities; the difference between believers who are probably right and those who are almost certainly wrong is that the authorities the first group listens to engage in practices and belong to institutions that are explicitly designed to sift truths from falsehoods.
These are truly astonishing statements. Entire books could be written about this paragraph. How can a Harvard professor derive his opinions from a “white coat” test? How can Pinker believe the authorities “explicitly” “sift[ed] truths from falsehoods” over the last few years but those not in power did not? This implies that on an extraordinarily broad range of emergent, complex topics there were no substantial disagreements among experts.
Let’s review what actually happened.
What if, as during Covid, comparably credentialed scientists in white lab coats argued opposite viewpoints? What if Group A in white lab coats, deploying superficial platitudes, proved consistently and stubbornly wrong about six or seven major items – virus origins, mortality rates, risk stratification, early treatment, lockdown harms, recovered immunity, and vaccine efficacy? What if Group B, also in white lab coats, deploying exquisitely specific analysis of biology and data, while demonstrating humility and a willingness to learn, often debating among themselves, proved mostly correct about those same six or seven major items? What if members of Group B had also offered testable predictions, which later proved true?
Because of Covid censorship and propaganda (CCP), however, Pinker was only exposed to Group A. He doesn’t even know Group B exists. Nor does he know about or value important contributions from Analysts and Physicians C, D, E, and F, etc., who may or may not have been wearing white lab coats but who offered crucial facts, data analysis, and front-line testimonies. Pinker thus confidently trusts Group A over what he believes to be know-nothing honkytonk yahoos on the interwebs.
As Stanford’s Jay Bhattacharya pithily summed up, Covid censorship created the “illusion of consensus.”
The result, as we wrote in early 2022, was that many of the Canadian truckers literally knew more about the deep biology of Covid than Pinker and the rest of the mainstream public policy community. Pinker had outsourced all his views on an array of extraordinarily complex topics to the Group A echo chamber. They turned out to be catastrophically wrong, many times over. The truckers, meanwhile, worked hard and dug deep, finding better data and arguments from experts B, C, D, E, and F. Now, three and a half years later, Pinker is still comprehensively uninformed about the molecular evidence which points, nearly definitively, to an engineered origin of SARS2.
The Crisis of Credulity
As we finished writing this article, economist Tyler Cowen credulously promoted a study claiming China suffered nearly two million excess deaths in just two months following the recent lifting of its zero-Covid lockdowns.
Tyler claims China would have succeeded if only they’d stayed locked down until they embraced mRNA vaccines. But he doesn’t address the morbidity and mortality surge across the high-income mRNA-consuming world.
The paper, published in the Journal of the American Medical Association, used an index of Internet searches and obituaries from three universities and then aggressively extrapolated an estimate for the whole nation.
This cohort study analyzed published obituary data from 3 universities in China (2 in Beijing and 1 in Heilongjiang) and search engine data from the Baidu index (BI; weighted frequency of unique searches for a given keyword relative to the total search volume on the Baidu search engine) in each region of China from January 1, 2016, to January 31, 2023. Using an interrupted time-series design, analyses estimated the relative change in mortality among individuals 30 years and older in the universities and the change in BI for mortality-related terms in each region of China from December 2022 to January 2023. Analysis revealed a strong correlation between Baidu searches for mortality-related keywords and actual mortality burden. Using this correlation, the relative increase in mortality in Beijing and Heilongjiang was extrapolated to the rest of China, and region-specific excess mortality was calculated by multiplying the proportional increase in mortality by the number of expected deaths. Data analysis was performed from February 10, 2023, to March 5, 2023.
China has been notoriously opaque and deceptive about its Covid health data. Observing a spike in “mortality-related terms” on the Baidu search engine (China’s version of Google) cannot make up for transparent, specific, reliable data. Perhaps one could generate a low-confidence hypothesis using this method. Asserting huge causal effects on such a flimsy basis is – what’s the word? – ridiculous.
Highlighting such a study is especially galling because Tyler avoids the rock-solid evidence of unprecedented excess mortality in far more transparent high-income nations.
More than a decade ago, Tyler’s Great Stagnation thesis jolted many in the technology world out of a long complacency. Contrary to industry cheerleading, he said, the pace of technological advance in most fields in recent decades had actually lagged both previous eras and our potential. Innovation is not automatic. We could do much better. He was right. Now, we are making big advances in transportation (EVs), space (SpaceX), A.I., and materials science (graphene), to name a few. If we want biotech to achieve its vast potential, we’ve got to be honest. Optimism requires critical, often unpopular, appraisal.
Comments on State Capacity Covidology
The One Million Lives Saved Claim: Part 1
Double Down Hallucination: Part 2
Who Really Wanted to Speed Remedies?: Part 3
Defending Steph Curry: A Computer Model: Part 4
Where Did All the Workers Go?: Part 5
A Narrative That’s Too Big To Fail: Part 6
Mortality Play: 2020 vs. 2021-22: Part 7
Japan Matches Germany's 2022 Mortality Spike: Part 9
Society of Actuaries Shows Continued Young Adult Mortality Spike: Part 10
Dr. Hotez’s Data Is Highly Flawed: Part 11
Covid and the Golly Folly: The blind spot of gee whiz technology futurism: Part 12
This is a mostly sensible summary. Unfortunately, Hanania’s detailed analysis and later conclusions don’t fit or follow from it.
The tightrope of progress means that in the world of public policy there are so many ways things can go wrong, and usually only a very narrow path to the desired location. You must avoid the kind of risk-aversion and safetyism elites seem prone to, and also being swamped by populist stupidity, with its distrust of anything new or different. It’s a miracle anything good gets done, and when it does, we have to be unequivocal in defending legitimate policy accomplishments.
What has really annoyed me about the public health community is that they sort of miss the whole point of public health. It’s not just to save as many lives as possible regardless of costs, otherwise nobody would ever go outside. It’s figuring out the rare targeted interventions that can make a large enough difference to be worth it. Economists seemed to understand this much better than epidemiologists.
UK data enjoys the advantage of a unified NHS. Government medicine suffers many shortcomings, but its ability to collect and analyze data comprehensively can be a strength. In this case, the UK has far better data about individual vaccination status, and its linkage to individual health outcomes, than the U.S. As we described in this article, the U.S. CDC miscounts both the numerator and the denominator in several ways, leading to completely useless or misleading effectiveness analyses. The UK is not perfect. It likely undercounts the number of unvaccinated Brits, perhaps by as much as 100%. The blue unvaccinated line in the chart above should in reality therefore be lower than the one displayed. The chart is thus the very best case in favor of vaccine effectiveness.
Professor Buckhaults also just testified for 30 minutes before the South Carolina Senate on the DNA contamination of the mRNA vaccines. Video here.
We could go on forever with accumulating evidence. The Australian has now reported that as early as April 2020, the medical intelligence arm of the U.S. Pentagon had already, through molecular analysis, determined SARS2 was engineered. Yet the U.S. intelligence apparatus blocked this knowledge from the public and even stripped it out of the August 2022 official report issued by the Biden Administration.
In just the last few days, a whistleblower, who is a senior CIA officer, told Congress that six of his seven-member team, charged with assessing the origin of SARS2, had initially concluded humans engineered the virus in a lab. But then, he alleges, his teammates were paid to change their minds and say they favored the zoonotic explanation.
UPDATE: On September 19, 2023, the the National Institutes of Health banned any more funding to the Wuhan Institute of Virology for 10 years. See letter.
Came over from Brownstone. Truly shocking how smart people can be so ignorant. And how so called scientists can blithely ignore evidence that refutes their claims.
I wondered what is it but I am sure now, that this is new ideology, it has nothing to do with science, truth or public policy. It's new religion based on marxism, depopulation, climate change doom and supporting for one government lead by corporations.
It's corporatism with depopulation together. The promise is, if we continue to support you to kill, rob others you will give us money, power and influence. We will lay and do whatever you tell us, just if you promise us to give us share from the new wealth and power you stolen from others.