


Who Really Wanted to Speed Remedies?
Comments on State Capacity Covidology: Part 3

Yes, I’m speaking of Covid-19 remedies. And while we’re at it, who really better understood infection fatality rates (IFR), "herd immunity," and escape mutants?
George Mason economists Tyler Cowen and Alex Tabarrock wonder if the scientists who favored a “focused protection” approach to Covid-19 truly care about old people.
If you didn’t follow the George Mason School of Covidology, Tyler writes, “you were not doing much to protect the vulnerable.” That’s odd. Because the U.S. and much of the developed world followed their playbook, and the result was one of the West’s biggest public policy disasters.
The George Mason scholars are most pointedly criticizing what might be called the Stanford School of Covidology, led by Drs. Jay Bhattacharya, John Ioannidis, and Scott Atlas. The Stanford School opposed mass closures of businesses, schools, and most institutions and instead urged “focused protection” of the vulnerable, especially the elderly. Protecting the vulnerable also meant shielding children and the poor from the devastating impacts of blanket closures. Drs. Bhattacharya, Martin Kulldorff, and Sunetra Gupta outlined the basic approach in the Great Barrington Declaration.
The GBD, however, was not their only or last word. The Stanford School was open to new data, new ideas, and new collaborations with physicians and scientists who were learning about new treatments, new protections, and the novel vaccines. The George Mason School, meanwhile, rigidly stuck to the plan of the Western public health authorities – lockdown indiscriminately, do not treat early, do not differentiate according to risk and benefit or clinical observation, vaccinate everyone maximally, and demonize those who disagree.1
The State Capacity Critique
Let’s reprint Tyler’s post and then respond.
Yes I do mean during the Covid-19 epidemic. As a follow-up post to Alex’s, and his follow-up, here are some of the effective measures in protecting the vulnerable, or they would have been more effective, had we done them better:
1. Vaccines, including speedy approval of same.
2. Prepping hospitals in January, once it became clear we should be doing so. That also would have limited lockdowns! And yet we did basically nothing.
3. Speeding up and improving the research process for anti-Covid remedies and protections.
4. First Doses First, when that policy was appropriate, among other policy ideas (NYT).
5. Effective and rapid testing equipment, readily available on the market.
If you were out promoting those ideas, you were acting in favor of protecting the vulnerable. If you were not out promoting those ideas, but instead talked about “protecting the vulnerable” in a highly abstract manner, you were not doing much to protect the vulnerable.
And here are three actions that endangered the vulnerable rather than protecting them:
5. Publishing papers suggesting a very, very low Covid-19 mortality rate, and then sticking with those results in media appearances after said results appeared extremely unlikely to be true.
6. Maintaining vague (or in some cases not so vague) affiliations with anti-vax groups.
7. Not having thought through how “herd immunity” doctrines might be modified by ongoing mutations.
Keep all that in mind the next time you hear the phrase “protecting the vulnerable.”
Most of these points are, to be kind, off base.
The Great Barrington Declaration doctors, Tyler’s most obvious targets, explicitly favored vaccination of the elderly and viewed it as a key component of “focused protection.” It would have been vastly preferable if we’d concentrated the vaccines on this population.
Prepping hospitals? Of course. But what does prepping hospitals look like? Apart from a few locales, hospital capacity was never the most crucial limiting factor of treating Covid-19. It would have been far more important to even more quickly (a) pivot away from ventilators as a first-line treatment; (b) adopt Dr. Pierre Kory’s protocol of corticosteroids and anti-coagulants to combat inflammation and clotting; (c) avoid the devastatingly toxic effects of Remdesivir, which Dr. Anthony Fauci quickly anointed the hospital “standard of care” despite contrary evidence, and which funneled billions of dollars to health systems despite widespread patient harm; (d) listen to world class critical care physicians like Paul Marik and Joseph Varon, whose ICU treatment regimen was three to four times more effective than the Fauci “standard of care,” but was blocked by devilish health system administrators responding to harmful Medicare incentives.2 Later on, vaccine mandates significantly reduced the hospital labor force, as nurses, staff, and even some physicians quit or were fired. In this way, State Capacity Covidology reduced hospital capacity.
Yes, if only. Early treatment of Covid-19 would have kept most people out of the hospital and saved hundreds of thousands of lives. But we did just the opposite. In the spring of 2020, the FDA blocked access to the national stockpile of 60 million doses of hydroxychloroquine. The Lancet published, then retracted, an outright fraudulent study seeking to undermine HCQ. The study was highly influential in the medical world, and by the time it was withdrawn, the damage had been done. Even if HCQ were only modestly effective, that’s not “speeding remedies.”
When we found an even better remedy – ivermectin – public health waged an even more vicious and underhanded war against it. In the medical journals, media, hospitals, and pharmacies. The doctors who treated patients most successfully with these and other well-known drugs and supplements were ferociously slandered and drummed out of hospitals, practices, medical societies, social media, and public life.
The “research process for Covid remedies” includes frontline doctors trying therapies and finding what works. Drs. Bryan Tyson and George Fareed in California’s Imperial Valley found success early on but were soon marginalized. They’ve now seen 20,000 Covid patients, with zero deaths among those treated within seven days of onset. World-renowned cardiologist Peter McCullough published early and often on emerging protocols which seemed highly effective. Doctors around the world read and implemented his evolving advice, until…
The FDA, NIH, CDC, WHO, and the entire State Capacity community launched an unprecedented full-spectrum assault on widely available, cheap, super-safe, generic drugs, which, as it turns out, were quite effective. These drugs are offered over-the-counter in many nations around the world. With their extraordinary and well-understood safety profiles, what could possibly have been the risk of widespread distribution? These didn’t need to be miracle cures. Even modest effectiveness would have recommended broad usage. Why don’t the George Mason economists praise the courageous doctors who saved thousands of lives in the face of overwhelming State Capacity interference? Why don’t they criticize the people and institutions which blocked access – not speeding remedies, but slowing them?
The huge volume of studies suggesting IVM and HCQ effectiveness were too persuasive.3 Opponents needed a counterpoint. To bolster the media war against these treatments and doctors, two influential studies – the TOGETHER and ACTIV-6 trials – were designed to fail. Here is Alexandros Marinos’ comprehensive multi-part series analyzing the defects of the TOGETHER and ACTIV-6 trials. Here are Charles Hooper and David Henderson on TOGETHER. And here is Yale epidemiologist Harvey Risch recounting the infuriating story of remedy suppression.
Tyler talks about speeding remedies in a highly abstract manner. But are the George Mason economists even aware of Drs. Risch, McCullough, Kory, Marik, Tyson, Fareed, James, and Talley, among hundreds of other unsung speedy treatment heroes? Do they know that Dr. Robert Malone’s earliest efforts, in January 2020, were focused on quickly finding and delivering “treatments and protections” and that he has an ongoing clinical trial?
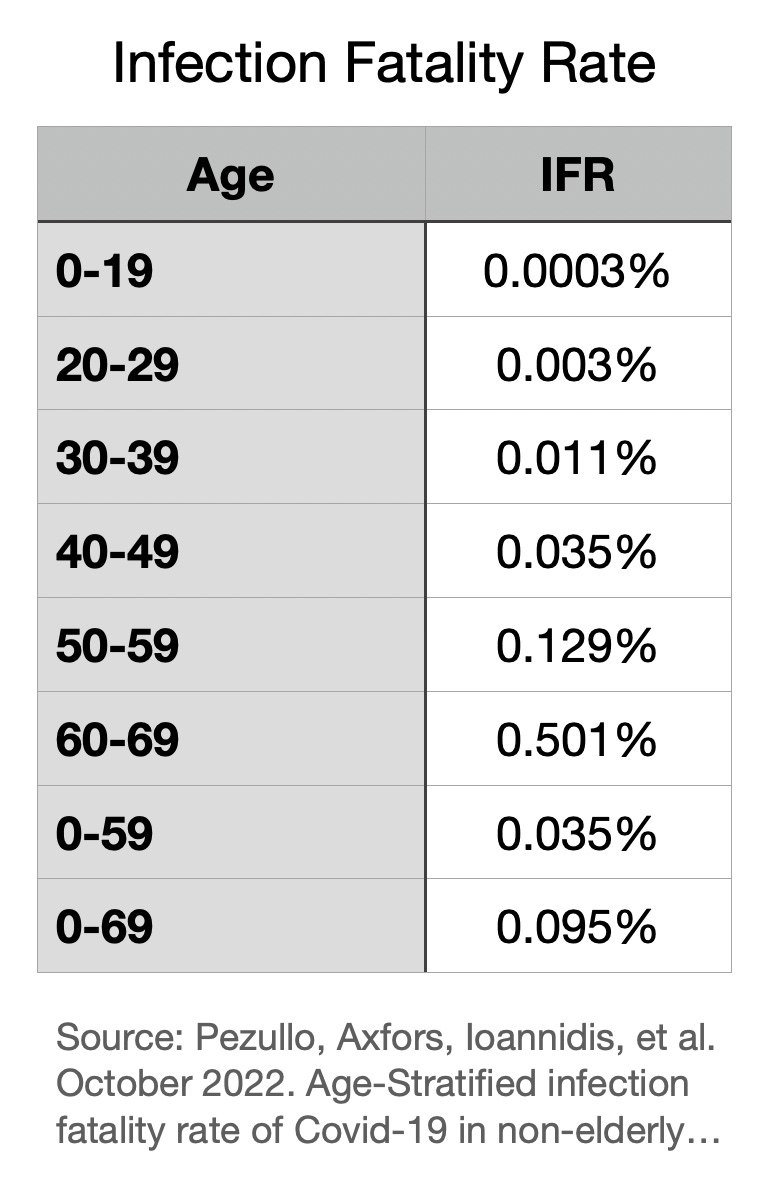
In April 2020, Stanford’s Jay Bhattacharya published one of the first seroprevalence studies, which estimated an infection fatality rate (IFR) of around 0.2%. That is close to where we’ve ended up. Stanford’s John Ioannidis’ latest compilation of worldwide data suggests an IFR of around 0.15% – much higher for older people, much lower for the young (see below). So why would it have been wrong for Bhattacharya to “stick[] with those results” when they kept appearing to be true? The inability to acknowledge Covid’s real world IFR and extreme risk differential between old and young is, to this day, a signal failure of public health and its State Capacity cheerleaders. The Imperial College models launched a panic in the spring of 2020, and its funders and adherents never corrected course when the mortality estimates proved wildly wrong. Three years later, the State Capacity crew can’t stop promoting models of pure fantasy.

This guilt-by-association statement about vague, or not so vague, affiliations with “anti-vax groups,” is itself vague. What’s the specific charge? By the way, why are the George Mason economists maintaining vague (or not so vague) affiliations with fantasy modelers, child-abusing lockdown enthusiasts, and early treatment deniers? Sounds pretty bad.
Tyler does not seem to have thought through how mass inoculation with a narrowly targeted, leaky vaccine during a pandemic might modify herd immunity doctrines. Why, for example, is uber-boosted Japan – at 2.99 doses per capita – now suffering its worst ever rise in Covid cases and deaths? As we wrote in November 2021, escape mutants may not be an exogenous shock but an endogenous result of extreme evolutionary pressure exerted by billions of vaccine doses targeting one part of the virus. In other words, our own interventions drove more rapid mutation and convergence on highly infectious variants which evade vaccine protection. Immune imprinting then locks the population’s immune profile on an extinct variant, while immune tolerance can downshift the immune response altogether. As we wrote earlier today, “Instead of achieving herd immunity by virtue of mass recovery from natural infection, mass vaccination using these technologies produced herd opportunity for the virus.” (See, More Vaccine Doses, More Covid Infections). The Wall Street Journal has caught on, too. See Allysia Finley’s January 1, 2023, article: Are Vaccines Fueling New Covid Variants?
A General Rule: the closer one is to Washington, D.C. (or other national or state capitals), the worse one’s Covid analysis.4
The Stanford School and its array of loose affiliates do not agree with each other on every topic or detail in the sprawling Covid universe. Many of them will disagree with portions of this analysis. But Stanford School adherents display several virtues: an understanding of basic public health and economic principles, appreciation for real-time feedback and distributed decision-making, and a willingness to listen and learn.
The George Mason School, on the other hand, abandoned its Hayekian roots and adopted the politico-health bureaucracy’s top-down, one-size-fits-all approach. And with extravagant certitude, no less.
Their favored Covid-19 lockdowns, mandates, early treatment prohibitions – and censorship of alternatives to all three – resulted in soaring all-cause mortality and morbidity, continuing to this day.5 School closures devastated children and young adults, educationally and psychologically. Clampdowns on work and production, combined with $10 trillion in spending to “replace” that lost output, is as textbook a case of stagflationary economic policy as one could imagine.
Tyler and Alex have taught and inspired several generations now. Daily, they enrich the public debate and enliven our conversations.
When it comes to Covidology, however, the Stanford School continues to trounce the George Mason School.
Comments on State Capacity Covidology
The One Million Lives Saved Claim: Part 1
Double Down Hallucination: Part 2
Who Really Wanted to Speed Remedies?: Part 3
Defending Steph Curry: A Computer Model: Part 4
Where Did All the Workers Go?: Part 5
A Narrative That’s Too Big To Fail: Part 6
Mortality Play: 2020 vs. 2021-22: Part 7
Japan Matches Germany's 2022 Mortality Spike: Part 9
Society of Actuaries Shows Continued Young Adult Mortality Spike: Part 10
Dr. Hotez’s Data Is Highly Flawed: Part 11
Covid and the Golly Folly: The blind spot of gee whiz technology futurism: Part 12
We apologize to George Mason professors Todd Zywicki and Don Boudreaux, who are in fact stalwart proponents of the Stanford School approach. GMU’s Bryan Caplan continues to chart a path between the two.
For example, health systems received a 20% bonus payment on the patient’s entire hospital bill if they administered Remdesivir, an ineffective experimental drug wildly toxic to the liver and kidneys. It’s so toxic, it failed its trial against Ebola.
See a new study demonstrating one of ivermectin’s many salutary mechanisms of action – the prevention and reversal of hemagglutination (one form of clotting), which is caused by the Spike protein of both SARS2 and the Covid vaccines. Boschi, et al, SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects.
Exceptions to this rule include Stockholm and Tallahassee.
Deep dives on all-cause mortality and vaccine harms are still forthcoming in this series.