


Thank you, Dr. Wilson.
Debunk the Funk doubles down. We respond.

TLDR: Thank you, Dr. Wilson, for putting together the strongest counterargument because it shows there is none.1

In March, Dr. Bret Weinstein, Dr. Joomi Kim, and I published a 2.5-hour video review of the micro-biology and macro-epidemiology of the mRNA Covid vaccines. We were, in part, responding to Dr. Dan “Debunk the Funk” Wilson, who had challenged Weinstein on the bio-mechanisms, safety, and efficacy of mRNA technology. See the video and our 60-slide presentation here:
On Saturday, Wilson posted a 25-minute rebuttal. Michael Shermer, editor-in-chief of Skeptic magazine, quickly cited it on Twitter/X.2 But Wilson only made things worse. Navigating Wilson’s rhetorical maze is messy and tedious. For all you die-hards, I’m going to counter his assertions below in great detail. Beware, however: the fog and dust is getting thick.
If you want the bottom line: Wilson’s multiple attempts at counterargument, including six expert immunologists and a Nobel Prize winner, showed we haven’t missed anything important. Our thesis, based on first principles and mountains of evidence, appears stronger than ever. Yet the fact so many expert testimonials still falter so fundamentally suggests the state of The Science is even worse than we thought.
Defunk the Bunk
Here’s a list of Wilson’s claims and omissions, along with my corrections and refutations.
I.
Wilson dismissed the autopsy findings of German pathologist, Dr. Arne Burkhardt, because his findings had not been published before he died. (Burkhardt was in the process of retiring when Covid hit and passed away in spring 2023.) We had summarized Burkhardt’s findings, performed with around 10 international colleagues and presented at several international conferences. Burkhardt and colleagues showed that among the examined 75 deaths soon after mRNA vaccination, at least 58 were vaccine-induced.
Wilson didn’t say Burkhardt’s autopsy findings were wrong – just that Burkhardt hadn’t published them in peer-reviewed journals before he died.
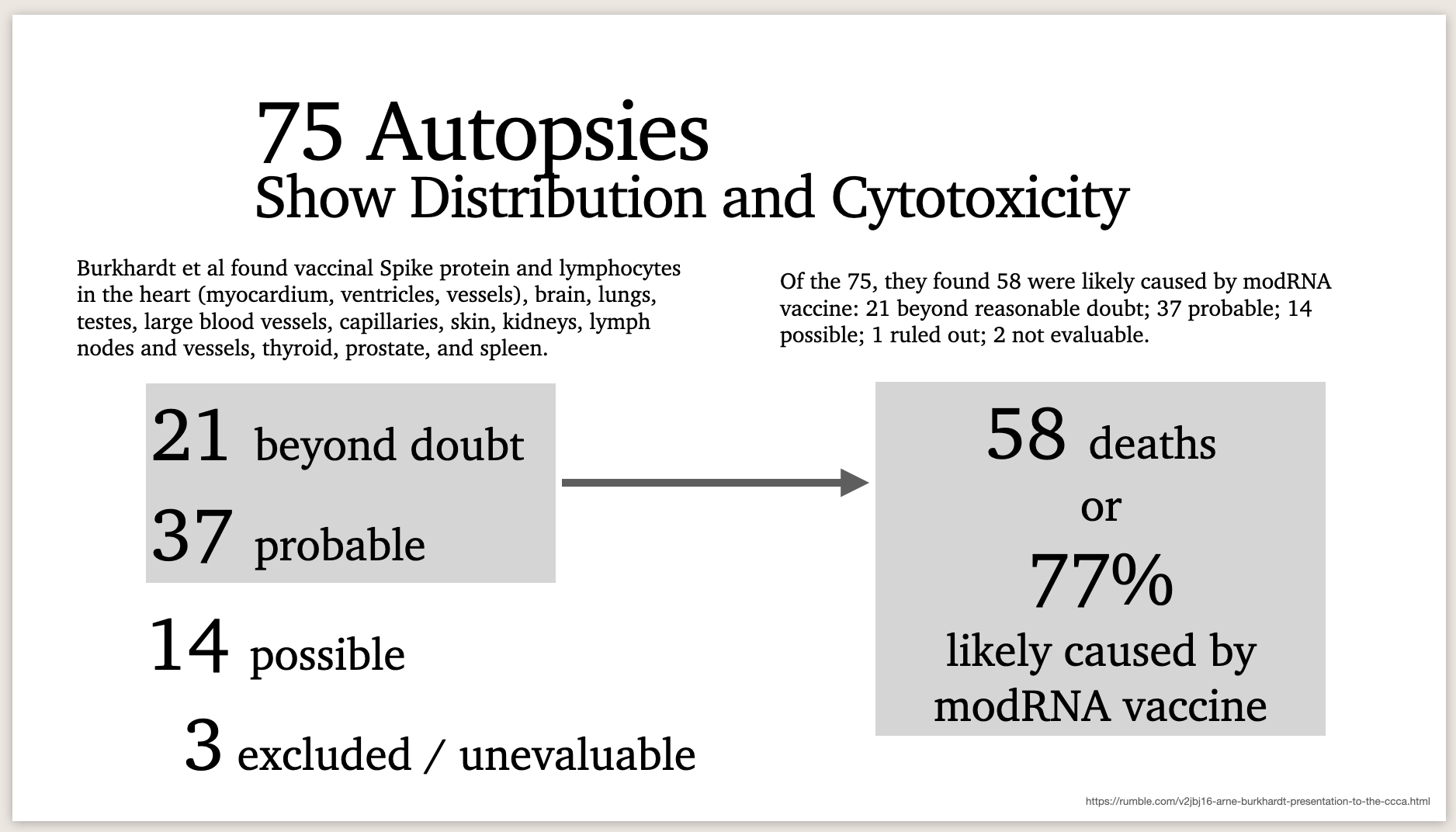
Wilson didn’t address the other autopsy and biopsy case series we cited, which confirm Burkhardt’s work. We highlighted published autopsy/biopsy papers by Schwab and Shirmacher, Gill, and Baumeier, among others, which demonstrated the exact mechanism of Spike expression and lymphocytic infiltration in the crucial damaged tissues that Burkhardt noted.
II.
Wilson doubled down on his baffling interpretation of a paper that both we and his experts cited. The paper – Cytokinopathy with aberrant cytotoxic lymphocytes and profibrotic myeloid response in SARS-CoV-2 mRNA vaccine–associated myocarditis – unambiguously bolsters our thesis of T and NK cell attack on cardiac tissue. It obliterates his experts’ bold assertions:
“There’s no evidence that there’s this massive immune response against the heart cells.”
“We don’t see…T cells targeting the heart. That has been looked at extensively. It clearly isn’t there.”
Yet Wilson attempts to muddy the waters by claiming the devastating volumes of mRNA-linked myocarditis are due to inflammatory cytokine reactions.
Well, yes. That’s what cytokines and chemokines do. Among other complex signaling traits, they warn of infection (in this case, transfection) and recruit cytotoxic T and NK cells to come attack invaded cells.
Here’s just one relevant passage from the paper in question:

One might say this paper doesn’t also specify modRNA in the heart; that wasn't its objective. So Wilson could argue the cytokine reaction is a general body-wide inflammatory response, which just happens to target the heart. System-wide inflammation is in fact an additional problem of the modRNA shots. But we know from many other sources, such as the Krauson et al paper we prominently cited, that modRNA “routinely” infiltrates heart tissue specifically and persists for at least 30 days.3 The cytokine signal is not merely general but specific.
Wilson’s pinning the cardiac damage on cytokines rather than T cells is like a defense attorney admitting to the jury his client painted the laser target on the murder victim’s forehead, and then asking the jury to ignore the gun and the bullet, which are also in evidence. Not an effective defense strategy. Regardless of one’s emphasis on cytokines or lymphocytes – we believe it’s quite obviously both – Wilson implicitly acknowledges, contra his experts, there is in fact a “massive immune response against the heart cells” and we do in fact see “T cells targeting the heart.”
III.
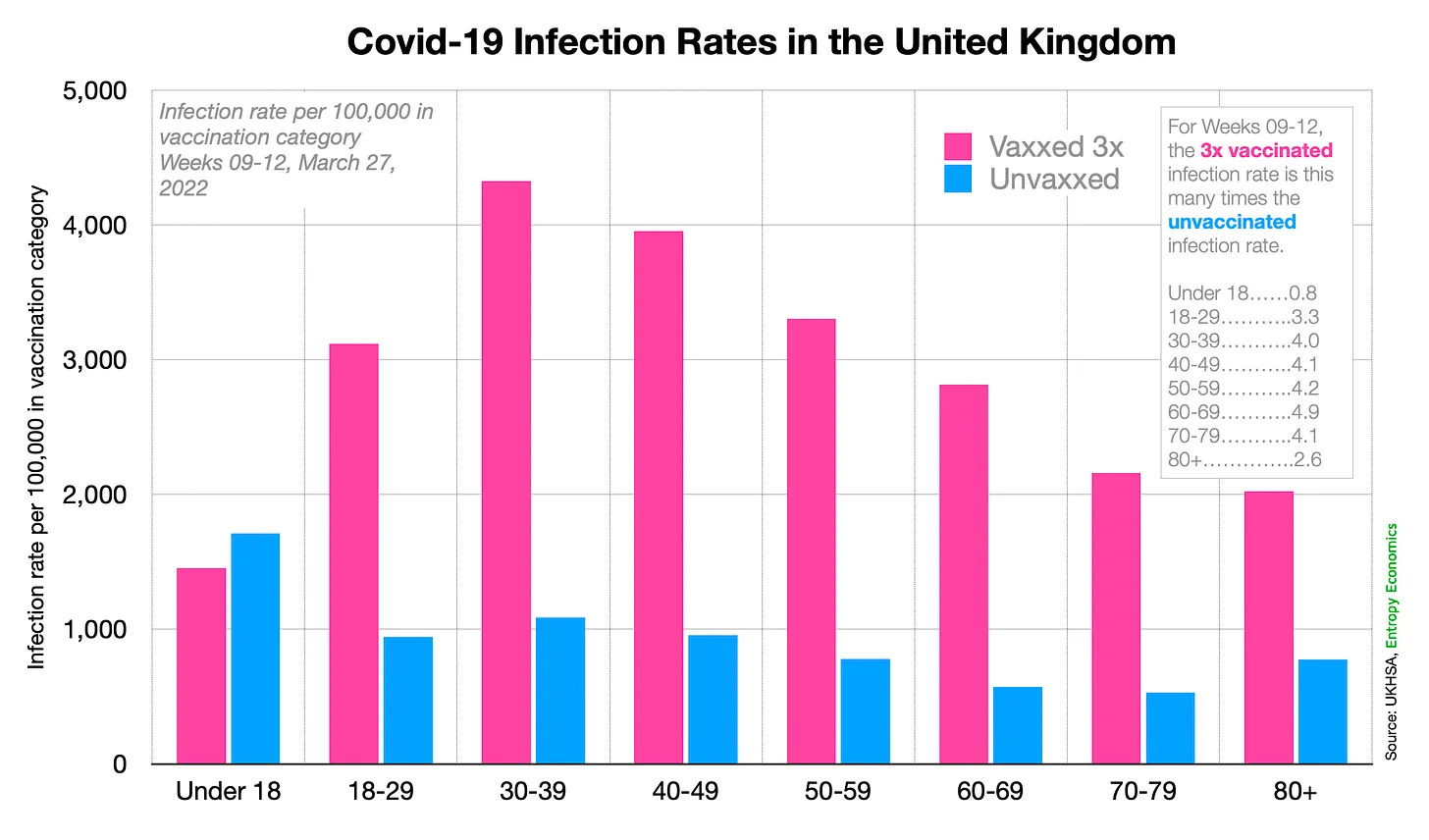
Wilson pulled a bait and switch on vaccine effectiveness. We showed why a famous chart his experts deployed was bogus. It relied on fatally flawed CDC data, which miscategorized vaccinated and unvaccinated people in at least three major ways – simple but systematic electronic record mistakes, the “two week black hole” where vaccinated are often considered unvaccinated until two weeks after the second shot (totaling around six weeks), and a large underestimation of the total unvaccinated population.
Wilson focused only on the two week black hole, which was in fact a major problem in numerous data reports and observational studies.4 Wilson simply denied the effect was real, but he’s simply wrong. See, for example, Norman Fenton’s many analyses5 and BMJ editor Peter Doshi’s paper, which criticized the “case-counting window bias” of nearly all observational studies:
“This asymmetry, in which the case-counting window nullifies cases in the vaccinated group but not in the unvaccinated group, biases estimates. As a result, a completely ineffective vaccine can appear substantially effective."
Wilson ignored the two other major problems – the simple record misclassification and the denominator deflation.
But he also pulled a card from his sleeve and switched from effectiveness – the argument of the chart – to safety, claiming all safety studies define vaccinated when the needle pierces the skin, thus slyly implying this bolsters the credibility of the effectiveness chart. If you’re not watching and listening closely, good magicians can fool you.
IV.
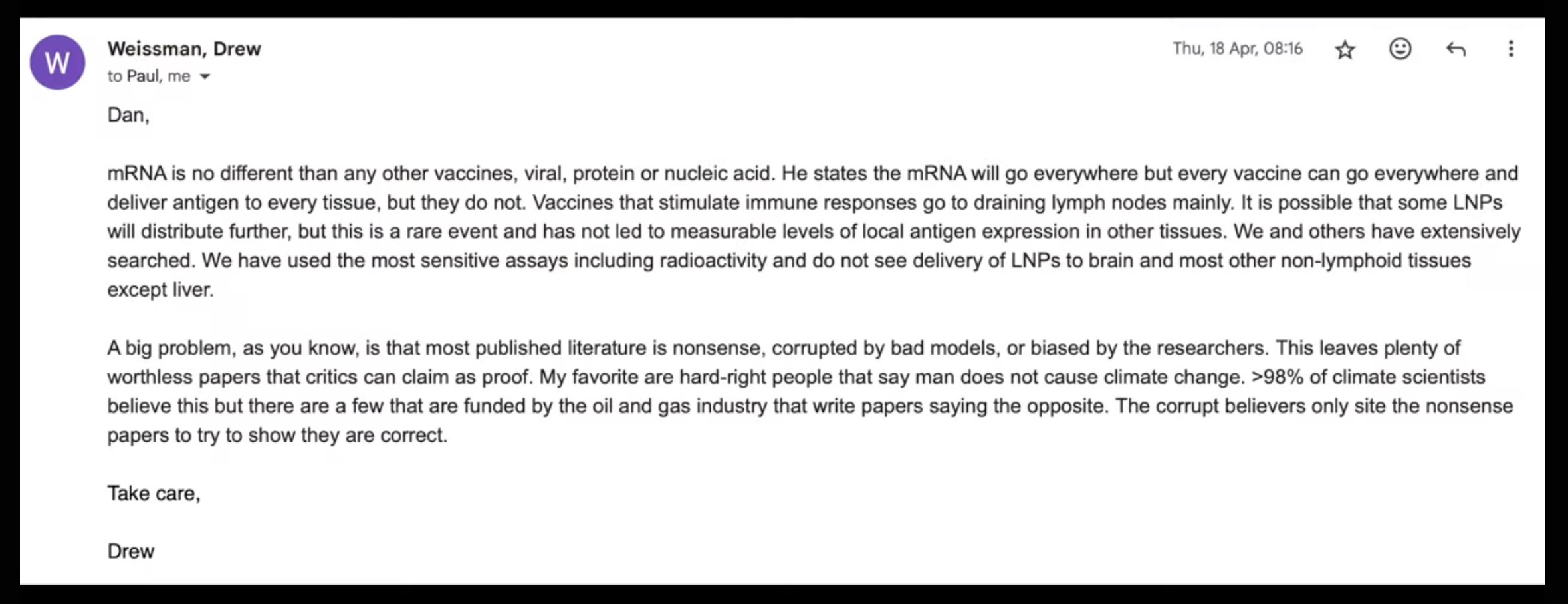
Wilson even solicited a statement from Dr. Drew Weissman, winner of the 2023 Nobel Prize for his addition (with Dr. Katalin Karikó) of N1-methylpseudouridine (m1Ѱ) to the mRNA recipe. This was the crucial step turning mRNA into modified synthetic RNA, or modRNA. Far from adding gravitas, Dr. Weissman’s statement alone is enough to capsize the credibility of the mRNA vaccines and the orthodox church of Covid. Dr. Weissman’s factual mistakes and overall obliviousness are jaw-dropping.
Nobel laureate Weissman made three bizarre claims, which must be unpacked because they each contain multiple misstatements and catastrophic cascades of illogic:
“mRNA is no different than any other vaccines, viral, protein or nucleic acid.”
“[Bret Weinstein] states the mRNA will go everywhere but every vaccine can go everywhere and deliver antigen to every tissue, but they do not.”
“Vaccines that stimulate immune responses go to draining lymph nodes mainly. It is possible that some LNPs will distribute further, but this is a rare event and has not led to measurable levels of local antigen expression in other tissues.”
First, if mRNA is no different than other vaccines, then why all the fanfare, including the Nobel Prize? Weissman is arguing he did nothing special. The fact is, modRNA encased in lipid nanoparticles (LNPs) is a radically new technology, at least in its first widespread human application. It differs from all previous vaccines and nearly all previous therapies in multiple, important ways.
Second, Dr. Weissman states that “Every vaccine can go everywhere and deliver antigen to every tissue, but they do not.” Can but don’t? Are we to believe every vaccine is allowed to spread through the body; they just choose not to? How does that work?
The fact is the LNP delivery system utterly changes the game. LNPs were designed to go everywhere and to efficiently enter cells, including difficult-to-access-areas such as the brain. Normal vaccine antigens, such as sub-unit proteins, do not enter most cells. Nor do they replicate. We know the dose and the half-life. We know exactly how much antigen enters the body, and that it does not transfect cells. A free-floating antigen can trigger the hoped-for antibody response (the humoral memory mechanism). But it does not interfere with delicate intracellular machinery, nor does it make copies of itself.
True, live virus vaccines do enter some cells and can replicate, but they are weakened to make them far less pathogenic, and our bodies have evolved to deal with natural viruses. Many of our tissues and bodily barriers resist natural viral infection.
LNPs on the other hand expertly spread and slip inside many cell types. Dozens of papers we cited contradict Dr. Weissman’s casual assertions that LNP distribution is a “rare event” and Spike is not “measurable” in tissues besides the liver and lymph nodes. Dr. Weissman relies on a few lab experiments with mice, but we now enjoy evidence from literally billions of human subjects, which he does not seem to have reviewed. In fact, hundreds of studies have measured substantial amounts of modRNA and/or Spike in the heart, lungs, kidneys, adrenals, brain, ovaries, testes, thyroid, prostate, spleen, skin, placenta, breast milk, and small and large blood vessels everywhere.
modRNA instructs our cells to produce the foreign antigen – in this case, Spike – and present it on the cell surface. Cells invaded by a non-self pathogen shoot up warning flares (remember those cytokines and chemokines). These signals attract cytotoxic lymphocytes, such as T and NK cells, to destroy the cells. If those cells are in your shoulder muscle, no big deal. If they are heart cells, very big deal.
modRNA, moreover, is not quickly digested like natural mRNA. Because of the 100% substitution of m1Ѱ for each uracil, based on Dr. Weissman’s research, the modRNA is far more stable. It can persist for months. And as long as it remains, the code can produce more antigen. The dosage, period of exposure, and location of expression are thus all unknown but potentially and dangerously too high and too broad. Dr. Weissman is surely a talented lab scientist, but he seems blissfully unaware of the mountains of varied evidence and data from the real world.
Dr. Weissman concludes his email to Wilson with a rambling statement about the scientific consensus over global warming, which does not inspire confidence.
V.
Wilson avoids numerous topics and major pieces of evidence which bolster our case and devastate his. In his now-deleted tweet, Michael Shermer said Wilson provided a “point-by-point” rebuttal. It was anything but.
Wilson evaded any discussion of our explicit refutations of his experts’ categorical denials of modRNA biodistribution and persistence. After we showed that his experts were dead wrong in their bold assertions on two of the central issues of this debate – biodistribution and persistence – he failed to counter our evidence. (See our 60-slide presentation.)
Wilson forgot to mention our discussion of negative effectiveness, as shown for example by the major Cleveland Clinic study, which has now been updated for the second time. Negative effectiveness was also eye-poppingly clear in the UK’s weekly reports until they discontinued them in spring 2022. The unfortunate fact is: the more modRNA injections, the more Covid infections.

He failed to address our discussion of autoimmunity, where we cited hundreds of papers demonstrating an endless array of perplexing immune dysregulations.
He avoided mention of ribosomal frame-shifting caused by m1Ѱ.
He ignored our discussion of IgG4 class-switching and tolerance.
He overlooked the 3,500 published case reports of serious adverse events we mentioned.
He never replied on the topic of DNA contamination.
Wilson glaringly dodged the most basic fact of all – the extraordinary excess mortality and morbidity observed in nearly every highly vaccinated nation in 2021-23. Unprecedented excess deaths were most conspicuous in young and middle-age healthy cohorts and are the single most inconvenient fact for those asserting modRNA safety and effectiveness. People all over the middle and high income world suffered worse health and higher mortality after the vaccines were introduced than before.

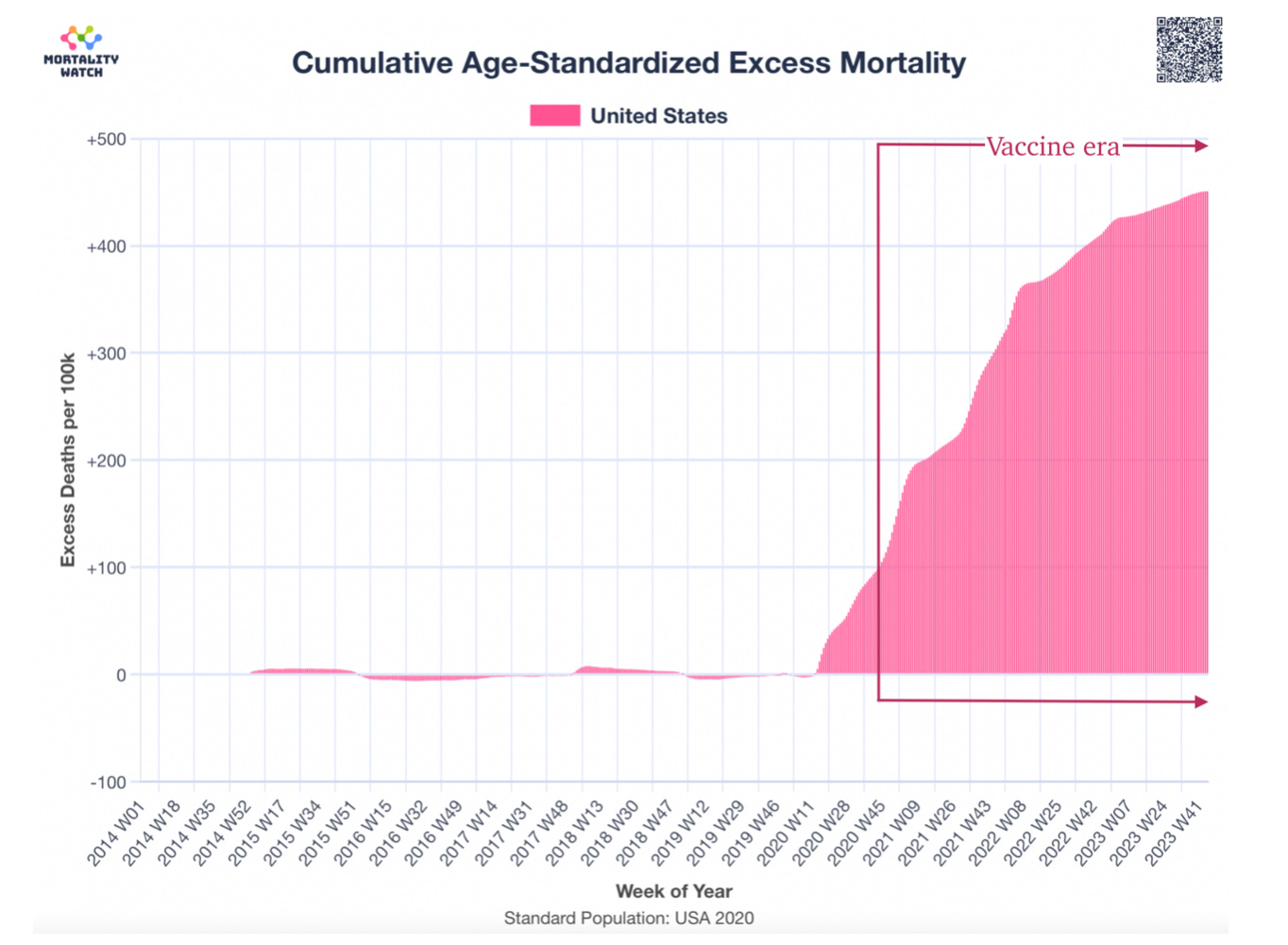
Wilson doesn’t and can’t deny these most important facts.
Courtesy of Alexandros Marinos.
Several days later, Shermer without explanation deleted the tweet.
“Vaccine was detected in the myocardium in a subset of patients vaccinated within 30 days of death. Cardiac ventricles in which vaccine was detected had healing myocardial injury at the time of vaccination and had more myocardial macrophages than the cardiac ventricles in which vaccine was not detected. These results suggest that SARS-CoV-2 mRNA vaccines routinely persist up to 30 days from vaccination and can be detected in the heart.”
Update on June 18, 2024: Yet another new effectiveness study employs the “cheap trick” / two week black hole.
From the paper: “Fourteen days after the second dose of Comirnaty (Pfizer/BioNtech), Spikevax (Moderna) or Vaxzevria (AstraZeneca/ Oxford University), or 28 days after a single dose of Janssen vaccine, status "Primary series - completed" started, in line with the requirements for the COVID-19 vaccination certificate [10]. Seven days after receipt of a booster dose, status "Boosted" commenced. https://www.sciencedirect.com/science/article/pii/S0264410X23006606
How long before sadly,cancer patients who take the new wonder drug die off in numbers.
Just to add to the squillions of papers ignored by Dr Wilson - I just read this one: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-024-17803-8
It looks at all-cause mortality in 29 countries from 2015-2022 and attempts to uncover factors associated with the rise in excess mortality over 2021-2022.
Factors which were positively associated with excess mortality included:
- people fully vaccinated
- people partially vaccinated
- stringency index
Booster jabs were negatively associated with excess mortality. But could this be explained by the two week window following receipt of booster in which individuals are categorised as not-yet-boosted? If risk of succumbing to a vax-reaction (in addition to risk of catching covid) is highest in the two weeks following receipt, than this will lead to a 'bump' in deaths in the 'people fully vaccinated' group, and a relative decrease in deaths in the boosted, right?
Bizarrely, this was the conclusion in the study:
"This study’s analysis of the factors influencing excess deaths suggests that effective strategies to mitigate all-cause mortality include improving economic conditions, PROMOTING WIDESPREAD VACCINATION, and enhancing overall population health"