


Free Novak Now!
Tennis all-timer Djokovic schools the world on Covid-19.

Novak Djokovic is better than everyone at tennis. He might also be better at science than the Food and Drug Administration (FDA) and Centers for Disease Control (CDC).
The United States is barring entry to all-time great Djokovic for the upcoming U.S. Open in New York. On July 10, Djokovic won his eighth Wimbledon championship and 21st Grand Slam title. It could have been his 22nd. But Australia blocked Djokovic from competing in the Australian Open in January, based on the fact he is not vaccinated for Covid-19. Now, the U.S. is doing the same.

The rationale for travel restrictions is similar to that of lockdowns and social distancing – to slow the spread. Vaccination is supposed to add yet another layer of protection. Travel and social contact while unvaccinated is – or was – thought to put others at risk.
The Infection Paradox
Two and a half years in, we know none of these tactics worked. Regardless of mitigation measures, the virus spread everywhere. If travel restrictions ever made sense for a highly contagious respiratory virus that had already escaped local containment and spread across much of the planet, they surely do not now. An unvaccinated Djokovic cannot contribute to viral spread in any meaningful way.
In, fact, a mountain of accumulating evidence suggests just the opposite: Vaccinees are now dramatically more likely than the unvaccinated to catch and spread the SARS-CoV-2 virus.
Evidence for this counterintuitive phenomenon began surfacing in the United Kingdom in August and September of 2021. Remember, Israel, the UK, and the U.S. had deployed the first large-scale Covid-19 vaccination programs beginning in the final weeks of 2020. The protective cover we all hoped for first cracked wide open in Israel in July 2021. Then the same happened in the UK and U.S. New waves of a new variant known as Delta showed the vaccines either suffered extremely short durability or could not protect against an evolved strain, or both.
The three countries rapidly decided to boost with a third shot, and much of the world followed suit. At the same time, however, we began to see a weird signal in the UK data.
It appeared as if vaccinees in some age cohorts were becoming infected at higher rates than the unvaccinated. Through the fall and winter, week after week, as the surveillance reports were published, the signal didn’t go away. It only grew stronger.

By January, compared to the unvaccinated, vaccinees in most age cohorts were around twice as likely to be infected. By March, that gap had blown out. And we had an additional surprise. The UK was now reporting unvaccinated versus the boosted, or triple-vaccinated. (Some speculate that the UK stopped reporting the double-vaccinated because those figures were even worse than the triple-vaccinated.)
In the last set of data released by the UK before it discontinued detailed weekly reports in March, the triple-vaccinated were 3-4 times more likely to be infected than the unvaccinated. Since then, negative efficacy has only intensified. Squabbles over the population data (NIMS vs. ONS) or behavioral effects on testing cannot make up for the gigantic signal. Evidence from around the world confirms the effect.

How is this possible? By now, everyone knows the vaccines don’t block infection or transmission. But how could they be worse than nothing? The probable answer is a phenomenon known variously as immune imprinting, or linked epitope suppression, or original antigenic sin (OAS). Our immune systems tend to be biased toward the first encounter with a pathogen.
Concentration Risk
When we first meet a bio-stranger, our immune systems identify the foreign organism or substance, or pieces of such, known as antigens. We mount a response – with innate antibodies, T cells, natural killer cells (NK), and then antigen-specific antibodies. After we clear the infection, we remember these antigens. If we see them again down the road, we recall the memory in our B cells, which reproduce the specific antibodies for those antigens.
It’s a beautiful and wildly complex system. But it’s not perfect, and we don’t understand it perfectly.
Foreign invaders evolve. If a similar but distinct strain comes along, we may recognize it. It may look familiar. It may recall our antigenic memories. But the antibodies we deploy based on our original engagement may not be perfectly matched to neutralize the new pathogenic cousin.
All is not lost, however. A natural infection produces a broad, diverse memory. A virus, for example, might contain a couple dozen protein antigens, which we size-up and produce antibodies against. Later on, even if one portion of a foreign invader has changed, we still have memories of its other antigens. This immune imprinting, therefore, may be only mildly suboptimal. Often, we’ve got antibodies aimed at other parts of the virus which may not have changed as much.
Unlike natural infection, the Covid-19 vaccines may imprint our immune systems in an especially acute manner. The vaccines contain mRNA1 instructions to produce a single antigen – the Spike protein.
In contrast with live-attenuated vaccines, for example, which might display the entire virus, or a large portion of it, with many antigens, the Covid-19 vaccines concentrated all their fire power on a single target of SARS-CoV-2 – the Spike protein of the original Wuhan strain.
(Robert Malone, pioneer of mRNA technologies, wrote about immune imprinting, with lots of citations, here: Immune Imprinting: Part I. Law professor Todd Zywicki wrote a sophisticated layman’s summary here: What is Original Antigenic Sin and Why Do We Care?)
Instead of educating our immune systems to recognize and neutralize multiple SARS-CoV-2 antigens, the vaccines trained us to fight only the Spike. Mass vaccination during a widespread pandemic with non-sterilizing shots put enormous, concentrated evolutionary pressure on the virus. Because of the exceedingly narrow target, the virus was offered a clear path to evade the vaccine: select for mutated Spikes which brush off the vaccinal antibodies. The evolutionary result was an explosion of highly infectious variants – Delta, Omicron, etc. – with massively mutated Spikes highly resistant to the vaccines.
A naturally infected person might fight off Delta or Omicron rather easily because they enjoy a broader immunity to these evolved variants. But a highly vaccinated person’s immune system has been trained repeatedly to respond only with the original Wuhan antibodies, which are now ineffective. Their immune systems have been pigeon-holed and sidelined.
A new Israeli study published in Clinical Infectious Diseases found that vaccinees were 13 times more likely to suffer an infection compared to unvaccinated people who recovered from natural Covid-19 infection. The vaccinees were also far more likely to suffer severe outcomes.

A new Qatari study found similar results:
Effectiveness of primary infection against severe, critical, or fatal COVID-19 reinfection was 97.3% (95% CI: 94.9- 98.6%), irrespective of the variant of primary infection or reinfection, and with no evidence for waning.
Canadian vaccinologist Byram Bridle wrote about the Israeli study and concluded that
naturally acquired immunity against SARS-CoV-2 is superior to the limited protection conferred by Pfizer’s mRNA product. This is just one of >150 peer-reviewed scientific publications that now confirm that natural immunity against this particular virus is better in every way to what can be conferred by the Pfizer shots. For me, as a vaccinologist, this is not at all surprising. Those of us developing vaccines always hold natural immunity as the gold standard.
The vaccines’ lack of antigenic diversity not only puts individuals at risk. It’s also the foundation of evolutionary escape at the population level. As in other arenas, lack of diversification leads to concentrated systemic risk.
Herd Opportunity
The previously infected, who enjoy robust if imperfect protection, are obstacles to viral replication. They contribute to herd immunity. The highly vaccinated, on the other hand, are fixated on a defunct variant and are vulnerable to recurring infections. They are easy prey and exert continued infectious pressure, promoting faster viral evolution. Unfortunately, they are obstacles to herd immunity. The virus thus enjoys more targets, a longer runway of replication, and thus increased potential to evade individual and population immunity. The vaccines are an unintentional gift. For the virus, they propagate herd opportunity.
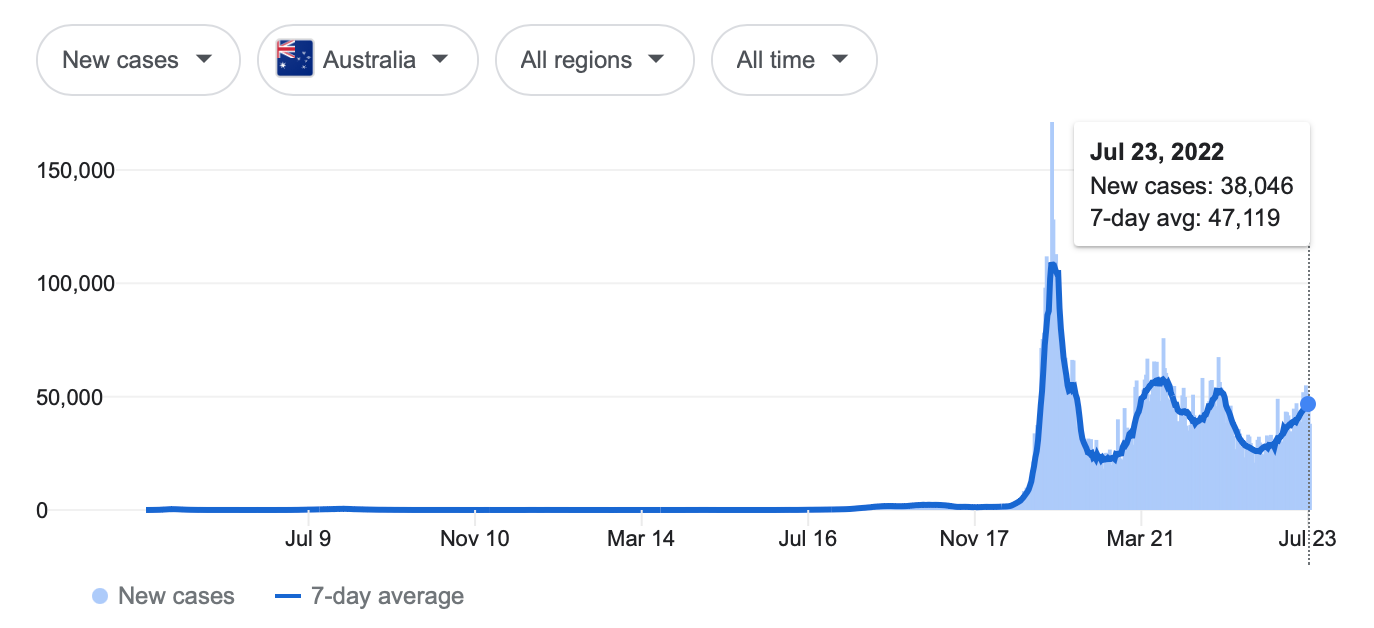
You can see this in the way the virus no longer comes in sharp waves, rising fast to a peak and then falling quickly toward zero. It no longer appears so seasonal, rising in winter, falling in summer. Instead, even after peaks, we see longer, continuous, moderate levels of infection. It simply doesn’t go away.



Pandemics often last six, 12, or maybe 18 months. They end when the population reaches herd immunity. Covid-19 is now past 30 months. Mass vaccination during a widespread outbreak appears not to have shortened the pandemic but prolonged it. It’s a dynamic which is difficult to grasp, and which all the modelers failed to anticipate. Now, many smart people are advocating another high-pressure campaign to boost yet again this fall. But the new tri-valent vaccines containing three Spikes – Wuhan and Omicron BA.4 and BA.5 – are likely to drive further imprinting and evasion.
A vaccine might protect some individuals against severe disease and death.2 And yet, if it does not sterilize against the pathogen – that is, block infection – it may still lead to more overall disease and death. If it unleashes waves of more infectious variants and also impairs the immune systems of vaccinees, it can radically boost the number of total infections over a longer period.
As you can see in the toy model below, a vaccine might modestly reduce the infection fatality rate (IFR). But if it supercharges total infections more than it lowers the IFR, the counterintuitive result can be more total morbidity and mortality.

Novak’s Easy Cost-Benefit Decision
Djokovic is young, supremely healthy, and thus at near zero risk from Covid. The vaccine won't meaningfully prevent him from acquiring or transmitting Covid and could possibly do the opposite. We have lots of generic treatments which neutralize Covid when taken early.
Novak’s direct risks from the Covid-19 vaccines, however, are not insignificant. These are radically new technologies, unlike any vaccines before.3 As FDA scientist Doran Fink acknowledged nearly a year ago, for men under 40 the risk of vaccine-induced heart damage alone probably overwhelms his risk from Covid-19. Myocarditis, which may strike around one in 2,500 or more young male vaccinees, is just the tip of the vaccine-injury iceberg (see Chua, et al.; Patone, et al.; and Sharff, et al.).
We now have 1,250 peer reviewed papers and case reports of vaccine-induced heart attacks, strokes, cancers, emboli, and a wide range of neuropathies, autoimmunities, and immune suppression. The German health ministry last week acknowledged one serious adverse event per 5,000 doses. Athletes are collapsing and dying at apparently unprecedented rates. We also see new waves of non-Covid respiratory infections which persist – colds and flus, for instance, which do not clear for many weeks.
A new reanalysis of the original Pfizer and Moderna trials demonstrates that even those shortened, best-case scenarios could not demonstrate overall benefit. Serious adverse events due to the vaccines outnumbered Covid-19 hospitalizations prevented.

Djokovic is engaged in a battle of science versus stubbornness. His decision to avoid the vaccine is rational and ethical – at least from a health perspective; it may cost him a few Grand Slam titles. He is protecting his fellow humans by refusing to participate in herd opportunity. The Australian and U.S. travel bans of the unvaccinated are worse than useless. At the extreme margin, they reduce immune diversity and promote spread of infection and continued, potentially dangerous viral evolution.
The mRNA contained in the first generation Covid-19 vaccines from Pfizer-BioNTech and Moderna should really be called something else – perhaps modRNA, syntheticRNA, pseudoRNA, or psiRNA. At the nucleotide level, they are not exact replicas of the mRNA of the SARS-CoV-2 virus. The vaccines make liberal use of N-1 methyl-pseudouridine, represented by the letter psi – 𝚿. RNA code employs four nucleotides – (A)denine, (U)racil, (G)uanine, and (C)ytosine. (DNA also contains A, G, and C but uses (T)hymine instead of (U)racil). In nature, pseudouridine 𝚿 can substitute for (U)racil at very low frequency – perhaps one or two percent of the U’s might be 𝚿’s. We don’t understand all the ways 𝚿 is a perfect substitute for U and how in other cases it might be a very imperfect substitute. In order to make the vaccines more stable and less inflammatory, Pfizer-BioNTech and Moderna replaced most of the U’s with 𝚿’s. This liberal use of pseudouridine perhaps worked in the ways they intended, but not without a number of unintended downsides. We will examine the potential problems of this synthetic RNA in future articles.
This oft-asserted “protection against disease and death” is far less clear than presumed. For example, 90.4% of all Covid-19 deaths in England in 2022 are among the vaccinated. Between August 2021 and May 2022, 85.2% of the Covid-19 deaths are vaccinated. See official data here. All-cause mortality – both Covid and non-Covid –also worsened in many high-vaccination nations in 2021 compared to pre-vaccination 2020. Also see a new analysis of the early vaccine RCTs, which found no overall mortality benefit for the mRNA vaccines. And of course, the excellent El Gato Malo weighs in here. Much, much more to say on this question.
The most prominent Covid-19 vaccines available in the West are novel. They are different from all vaccines that came before. Most “vaccines” as we knew them may be highly safe and effective, among medicine’s great inventions, and yet the new Covid-19 products may not be. Calling something a “vaccine” does not automatically confer infallibility. Take the Pfizer and Moderna products. They employ (1) a novel delivery vessel – the lipid nano-bubble; (2) a novel method of antigenic expression – genetic transfection of our cells with synthetic mRNA; and (3) a novel single-antigen payload – the Spike protein, which we now know is itself cytotoxic. We might expect that such a radically new genetic therapy, insufficiently tested at “warp speed” and deployed to billions of people, might produce some surprising outcomes for individual health and population dynamics.